Project Cardiogram
- India
- Nonprofit
The burden of cardiovascular diseases (CVD) in India is staggering, with annual deaths rising significantly over the past few decades. India faces an urgent need to address this crisis, particularly in rural areas where access to healthcare services is limited. The World Youth Heart Federation (WYHF) aims to tackle this issue by improving access to cardiovascular healthcare services in rural India through a comprehensive approach.
WYHF's strategy involves establishing scalable and sustainable cardiovascular healthcare referral and treatment services integrated with the public sector. This includes raising awareness about CVDs and their risk factors among the general population, leveraging Accredited Social Health Activists (ASHA) workers, and organizing community screening camps to detect CVDs and other non-communicable diseases like diabetes early on.
One major challenge identified is the lack of essential medical equipment, particularly ECG machines, in rural health centers. Despite national guidelines mandating their availability, a baseline assessment across 101 Peripheral Health Centres (PHCs) in Gujarat revealed that only two PHCs had functional ECG machines. Moreover, while healthcare workers in some PHCs were capable of taking ECGs, only a fraction had medical officers trained to interpret them.
To address this gap, WYHF's "Project Cardiogram" aims to deploy ECG machines at PHCs and provide training to healthcare staff for interpretation and management. Additionally, the organization is leveraging digital health and telemedicine to strengthen the referral system, ensuring timely access to care for patients, especially in emergencies like heart attacks.
Preliminary data from a pilot screening camp in Anand city, Gujarat, underscored the significance of this initiative. Out of 71 patients screened for cardiovascular risk factors, 21 showed abnormal ECG findings. This highlights the critical need for screening, training, and the deployment of ECG machines across PHCs nationwide.
Furthermore, the prevalence of hypertension in rural areas underscores the vast number of undiagnosed cases. Despite guidelines suggesting a prevalence of 18.1%, PHCs are falling short in identifying and treating hypertensive patients. This signifies the importance of proactive screening initiatives to bridge this gap in healthcare delivery.
In conclusion, WYHF's efforts to strengthen rural healthcare systems by improving access to cardiovascular healthcare services are vital in combating the growing burden of CVDs in India. Through initiatives like Project Cardiogram, the organization aims to equip PHCs with essential resources, enhance healthcare worker capacity, and leverage technology to ensure early detection and effective management of CVDs, ultimately saving lives and reducing the economic burden on society.
The Cardiogram project, initiated by the World Youth Heart Federation - India chapter, aims to narrow the healthcare disparity between urban and rural areas. Its objectives encompass assessing current healthcare systems, training healthcare workers to detect cardiovascular risk factors early, deploying Digital ECG machines at Primary Health Centers (PHCs), conducting community-based screening camps, and integrating digital health and Tele-Medicine.
Amid the COVID-19 pandemic's second wave, resources were redirected to COVID relief efforts through the Local Heroes Project, which focused on hyper-local assistance. This experience highlighted the need to strengthen rural healthcare, leading to the inception of Project Cardiogram.
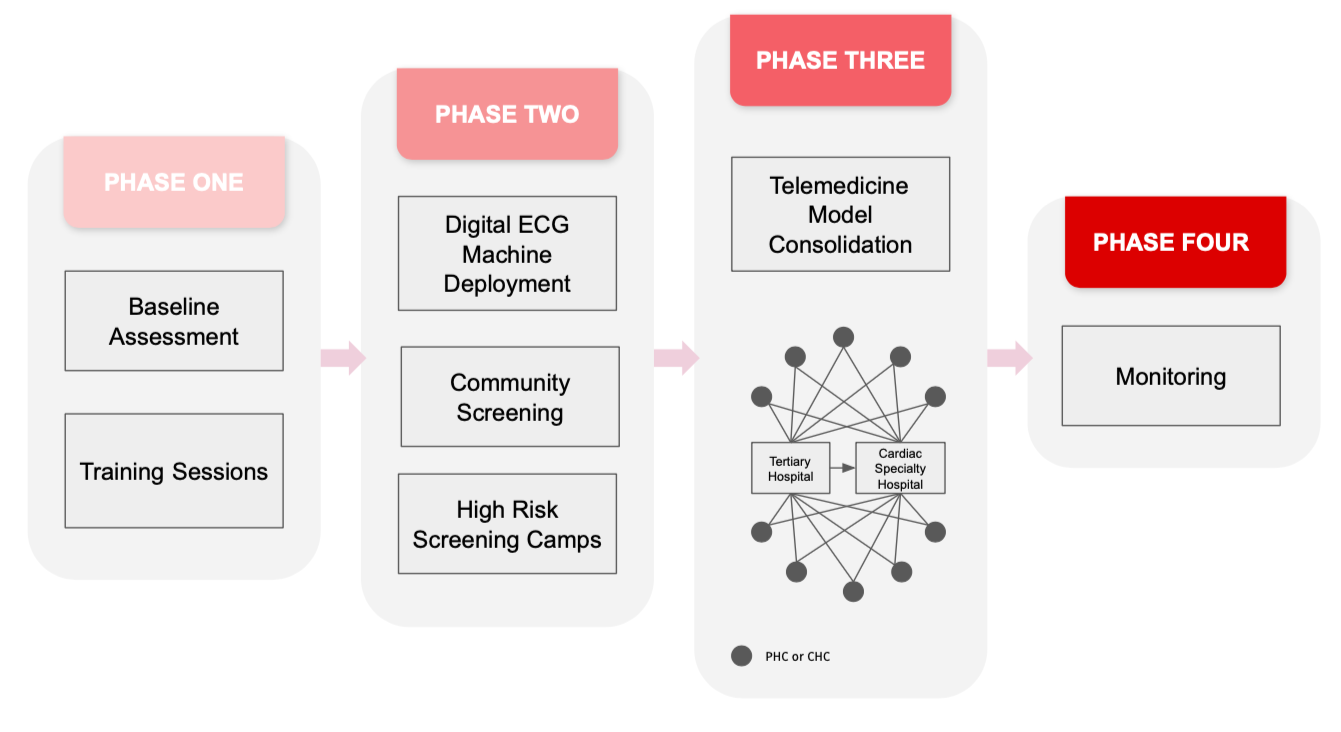
Derived from "cardio" (heart) and "gram" (village), Cardiogram emphasizes rural areas due to significant healthcare disparities. The project operates in phases, starting with needs assessment and research at 500 PHCs in Gujarat, prioritizing those lacking ECG machines. Training programs for healthcare workers follow, covering ECG interpretation, risk factor identification, and symptom recognition.
Deployment of ECG machines at PHCs is coupled with organizing screening camps for data collection and intervention. These camps raise community awareness of cardiovascular diseases and identify silent cases and risk factors. Currently, Digital ECG machines are being deployed, with 11 screening camps conducted.
Integrating ECG machines with telemedicine units establishes a "Hub & Spoke model." Primary healthcare facilities serve as spokes, providing initial patient contact and treatment. Routine patients receive care locally, while high-risk cases are referred to hubs for specialist consultation. Regular screening camps further aid in early detection.
Efficient referral services rely on vertical and horizontal communication between spokes and hubs. Tertiary care hospitals act as hubs, providing specialized treatment and admitting patients referred from spokes. A standardized public-private partnership agreement ensures quality care.
Telemedicine units at hubs interpret ECGs and guide local healthcare workers. While they cannot influence referral decisions for commercial gain, they offer clinical guidance. The functional capacity of telemedicine units varies based on available resources.
In the next year, Cardiogram aims to complete baseline assessments in Gujarat and expand to districts in Maharastra and Karnataka. Training 100 staff nurses and medical officers, deploying ECG machines on needs basis, and screening 5000 individuals are key goals. Establishing 5 district-level clusters with telemedicine facilities is also planned.
In summary, Cardiogram addresses rural healthcare disparities through systematic interventions, including training, equipment deployment, screening camps, and telemedicine integration. Its "Hub & Spoke model" ensures efficient patient referral and treatment, emphasizing collaboration between primary and tertiary care facilities. By focusing on capacity building and community engagement, Cardiogram strives to enhance cardiovascular healthcare accessibility and outcomes in underserved regions.
Our solution is focused on strengthening the Rural healthcare system that would directly impact the Rural population of our country which accounts for more than 65% of India's total population. Mainly our solution would serve the rural inhabitants as well as the rural healthcare workers. People living in rural areas do not have direct access to advanced healthcare facilities present at a Tertiary Care centre in urban areas due to reasons like poor connectivity, financial constraints, lack of awareness etc. and hence it is imperative to provide these people access to basic lifesaving healthcare facilities like ECGs in order to timely and effectively manage and thereby decrease the burden of cardiovascular conditions. The project also advocates for recognizing the systemic barriers faced, and prioritise inclusive approaches that address their unique needs and challenges of vulnerable groups.
For rural populations with different socio-economic backgrounds and different minorities, culturally competent healthcare services, including language-appropriate education and resources, to ensure equitable access and outcomes for accessible healthcare facilities, services, and information, alongside initiatives to train healthcare providers in disability-sensitive care. Young adolescents benefit from early intervention strategies targeting cardiovascular health, emphasising healthy lifestyle behaviours and access to nutritious foods.
Women and girls benefit from gender-sensitive approaches, addressing maternal health disparities and promoting access to health education and understanding how cardiovascular issues manifest distinctly than in men. By prioritizing equity in all aspects of project, we aim to dismantle barriers and create inclusive healthcare systems that promote the well-being and resilience of marginalized and vulnerable groups, ultimately fostering a healthier future for all.
Access to ECGs at a PHC level would help the individuals in getting early information on their condition which would lead to early and effective management and thereby decreasing the morbidity and mortality. Also, one major purpose of installing digital ECG machines is that the individuals would be able to have a record of their own ECGs with themselves. The ECG machines which we deploy at the PHC have the facility of sending a copy of ECG to the patients as well. This would serve as their baseline ECG and hence help the healthcare professionals in identifying any changes, if at all later, on subsequent examinations.
The availability of ECG machines at PHCs would also help in decreasing the burden of suspected cardiovascular disease presentation at the tertiary care centres by filtering the false positives at the primary and secondary care levels. Many times the patients present with cardiovascular symptoms like chest pain but have no underlying serious condition. These patients are unknowingly referred to higher centres due to unavailability of ECG machines and fear of a worst outcome, ultimately putting the patients through unnecessary travelling and financial loss.
Apart from that, presence of ECG machines would lead to inclusion of special cardiovascular disease prevention programs at the primary health centres which in turn would also create job opportunities for the people from the local community for positions like ASHA worker (Accredited Social HEalth Activist) and Anganwadi workers.
WYHF currently has a Volunteer network of around 600 medical students, junior doctors, and business professionals in all the states of India actively working on ground to bridge the rural-urban gap in Healthcare system and collaborating with other student organisations to achieve common goals. Our team has been working since the past 20 months, initially planning and establishing a framework to later on doing on-ground work to create an actual impact in order to understand the burden of problems from various perspectives. Our pilot project made us realise the intricacies which need to be focused upon and divert our attention towards prioritising the involvement of local community members like ASHA workers, Anganwadi workers and Female health workers (FHWs) to support us in achieving maximum community outreach and help us understand their difficulties and requirements better.
In our pilot studies we identified several factors that acted as hurdles for our project which include financial constraints, passive health seeking behaviour, fear of hospital admission, ignorance of severe health conditions etc. To address these concerns, both external support such as that being provided by WYHF or government schemes as well as internal support from the surrounding community is necessary.
The involvement of the local community comes at a very crucial stage of the project. After establishment of the desired system, it is equally important for us to maintain the same and hence, the involvement of community is very crucial to ensure sustainability. We plan to involve representatives from the locality nearby the respective PHCs or CHCs for ‘Monitoring’ of the project and they would be working together with the WYHF local team in ensuring proper chain of communication and smooth flow of the system. These representative individuals would be supported and trained with basic life skills and would be provided with opportunities for their own progress.
- Increase access to and quality of health services for medically underserved groups around the world (such as refugees and other displaced people, women and children, older adults, and LGBTQ+ individuals).
- 1. No Poverty
- 3. Good Health and Well-Being
- 5. Gender Equality
- 9. Industry, Innovation, and Infrastructure
- 10. Reduced Inequalities
- 17. Partnerships for the Goals
- Growth
In the past 2 years and 6 months, we have been able to serve more than 1.82 million (10 CHCs serving a population of minimum 50 thousand each and 44 PHCs serving a minimum population of 30 thousand each) people by deploying ECG machines at various Primary health centres (PHCs) and community health centres (CHCs) across the district of Vadodara and 2 PHCs in the district of Anand along with conducting community level screening camps. We have also been able to train more than 55 healthcare workers in ECG lead placement, identification of risk factors, symptoms and ECG interpretation.
Our goal at WYHF is to establish a scalable and sustainable cardiovascular healthcare referral and treatment service integration with the public sector to improve patient outcomes and also raise awareness regarding cardiovascular diseases and their risk factors among the general population. We believe that via the medium and support of Solve we can achieve this herculean task. Via your support, many previous projects working towards improvement of healthcare like projects for prevention of chronic diseases, projects for simplifying healthcare data recording, projects for digitalization and use of technology in healthcare etc. have been successful in implementing their solutions.
One of our biggest barrier is the development of a digital health solution. We are trying to create an online platform with a one stop solution for the majority of the information related to cardiovascular health and disease. For our project Cardiogram we aim to integrate Tele-Medicine and the Hub & Spoke model on this online platform wherein a group of expert healthcare professionals can come together to help patients get correct interpretation of ECGs and timely management and referrals in case of emergencies. This platform would also serve as a medium for storage of the collected data for Research purposes.
As we have a pan India presence, we also face several cultural barriers like differences in language of communication, cultural beliefs, level of education etc. and legal barriers such as ethical issues pertaining to data privacy, medical interventions etc. Major financial barriers include funds required for procurement of ECG machines for deployment at the PHCs and CHCs. We believe that with the support of Solve we can overcome these barriers and implement our solution at a national as well as global level.
- Business Model (e.g. product-market fit, strategy & development)
- Financial (e.g. accounting practices, pitching to investors)
- Monitoring & Evaluation (e.g. collecting/using data, measuring impact)
- Technology (e.g. software or hardware, web development/design)
The COVID-19 pandemic made people realise the increasing importance of healthcare but the involvement of only the healthcare workers in improving the healthcare of the society can bring very limited change which we aspire to see. Hence, we started this project at WYHF with an objective of intersectoral collaboration which is a new concept in the field of healthcare in our country. Project Cardiogram is an innovative solution to tackle the rising burden of Cardiovascular Disease in India with the use of digital health solutions and utilisation of telemedicine to provide diagnostic and therapeutic aid in rural areas, where there is scarcity of resources. With the use of digital health, we can provide the rural population with access to quality healthcare in an effort to move towards Universal Healthcare coverage.
.
The phased implementation of our Project enables us to take a systematic approach towards our solution and the work done at each step sets up the foundation for the subsequent steps. Baseline assessment would help us obtain actual data of ground reality which would in-turn help in policy making. Our countries' current diagnostics and management criterias are based upon data collected from foreign countries with populations very different from ours. The data collected via this project would help us bring changes in policies which are more suited to our population. Apart from that, the installation of ECG machines at rural centres will open further opportunities for digitalization of rural healthcare system as the government of India is also planning to bring healthcare cards for each individuals of our country which would help us incorporate a patients baseline cardiovascular health record through this project.
The conduction of community screening camps would ensure that our project not only helps in management of acute cardiovascular accidents, but also has long term benefits in reducing mortality due to CVD by early risk factor identification. The concept of ‘Hub & Spoke model’ is also a new and innovative solution to give access to people with advanced diagnostics and treatment options which were earlier only limited to the financially stable urban population. This intersectoral collaboration will not only benefit the rural inhabitants and healthcare workers but will also allow individuals from fields apart from healthcare to contribute towards betterment of the society. Digitalization of Healthcare would also open up opportunities in the IT & engineering sector, marketing & management sector, medico-legal sector etc.
Goals for the next year:
To provide access to ECG Machines to 10 million people by installing ECG machines at 500 PHCs in rural areas in four states of India namely Gujarat, Goa, Jammu & Kashmir and Assam.
To decrease mortality due to Cardiovascular Diseases by training 1000 staff nurses and medical officers at rural PHCs to use ECG machines, identify a normal ECG and perform cardiopulmonary resuscitation (CPR). Also, identification of cardiovascular symptoms and risk factors.
Establish 15 district level clusters including PHCs and higher referral centres with telemedicine facilities.
Screen 50,000 individuals for cardiovascular diseases and diabetes through community level screening camps.
Goals for the next 5 years-
Impact- Educate 3,00,000 patients in local languages about their CVDs; Support 5 cardiovascular health (CVH) startups; Publish 25+ relevant research papers; Advocate for implementation of project CardioGram (backed by cost effectiveness analysis study) by NDHM support; Procure 2 CVH tech patents; Provide access to 30 million rural inhabitants of India to digital ECG machines and in turn establishing telemedicine facilities at PHCs and CHCs to provide specialist cardiovascular healthcare facility; Screen 75,000 individuals for NCDs including CVDs and diabetes; Train 10,000 primary health doctors to provide emergency cardiovascular life support; Design an online platform that would serve as a telemedicine interface and increase the efficiency of the process and Save 5,000 lives.
Outreach- Mobilise 15,000 young individuals from diverse backgrounds to improve CVH; Establish 20 new National Chapters including LMICs from all 6 WHO regions; Collaborate with 30+ National and International NGOs to collectively achieve our goals.
We measure the impact we make at every stage of our project through needs assessment surveys and other questionnaires. At the preliminary stage we conduct a needs assessment at rural healthcare centres to assess the existing resources, population and healthcare worker characteristics to ensure that the deployment of an ECG machine would provide maximum benefit. Our training sessions are equipped with a pre and post session questionnaire to ensure that the training was successful and adequate.
The data collected in our community screening camps helps highlight high risk patients who would require further management. The collected data helps determine the impact of early detection and management on mortality rates due to cardiovascular disease. The individuals with high risk factors are followed up regularly at the PHCs to evaluate their treatment progress. The ECGs collected after deployment help assess the prevalence of cardiovascular disease in the community. The ECG manufacturers also provide us with weekly data on the usage of the machines and other factors like reporting turnaround time, number of referrals, individual location information, hub statistics for the entire cluster etc.
We present this report to the Chief District Health Officer (CDHO) who is the top most healthcare official for a district. Based upon the reports, the CDHO implements subsequent necessary changes which would help improve the outcomes of the project. Apart from this, we also plan to do a cost effectiveness analysis at each step of the project to help us use and divert (if necessary) the collected funds efficiently. For our previous project ‘The Local Heroes’ as well, we conducted cost effectiveness analysis with promising outcomes. Ultimately, a reduction in cardiovascular disease morbidity and mortality over time in the region of our presence will serve as the greatest impact for our project.
Our project mainly relies on digital health to provide the expertise of highly trained doctors in rural areas to identify and manage cardiovascular disease. We use digital ECG machines to record ECGs that are sent to doctors (from public or private hospitals) at the associated Tele-medicine units who can remotely provide the diagnosis and suggest steps for further management. These tele-medicine units would be incorporated onto a common web portal which would also provide educational material and access to other resources related to cardiovascular health to different groups of people including patients, healthcare professionals as well a general population.
Currently for ECG report transmission as well storage of data we are relying on external apps and communication platforms like WhatsApp but considering appropriate ethics involving data privacy and sharing we aim to be self sustainable and use less of the general/public platforms for future endeavours. We plan to incorporate block-chain technology for individual data privacy which would prevent misuse of the vast majority of the available data by monetary businesses for personal gains. In all, our purpose is to create a safe, secure, efficient and sustainable digital platform for logistics, administration and smooth implementation of our projects.
- A new application of an existing technology
- Artificial Intelligence / Machine Learning
- Audiovisual Media
- Imaging and Sensor Technology
- Software and Mobile Applications
- India
The WYHF boasts over 650 members and impacts over 25,000 students nationwide. Each project, like Cardiogram, mobilizes volunteers through specific calls. The National Team, led by project heads and coordinators, orchestrates efforts across regions. In Vadodara-Gujarat, a local team of 30, including a city lead, partnership head, research lead, and activities head, drives the Pilot project. They ensure smooth progress, secure sponsorships, execute data collection, and coordinate on-ground activities with healthcare personnel. This structured approach maximizes impact and fosters efficient communication between local and national levels, enhancing community health initiatives.
The idea behind this project came up during the 2nd wave of covid pandemic in India around June in 2021 wherein we realised the need for improving the inefficient and overburdened healthcare system. The planning and making of the project layout was initiated there onwards, following which the active ground work was started from August. In the subsequent 6 months we were able to cover the district of Vadodara-Gujarat including baseline assessment, deployment of ECG machines at various CHCs and setting up of integrated telemedicine units. Currently we are working towards baseline assessment of the districts across India.
The inception of WYHF was based on the concept of Intersectoral collaboration wherein people from different fields like medicine, engineering, business, designing, technology etc. come together to work towards a common objective of improving Cardiovascular health of the society. The idea behind this was to indulge with professionals and experts from various sectors to understand the problems better and thereby work towards implementing more effective strategies and solutions. Our focus is more towards empowering Youth to take up leadership roles and, aside from their personal development and profession, divulge some of their knowledge and energy towards the betterment of the society.
Our Pan India presence in each and every state of the country is representative of our geographic and cultural diversity. For administrative purposes we have divided India into 4 regions (North, South, East, West) with equal representation from each of these. Each and every member of the organisation is eligible for participation in any of the projects or activities taken up by the working committees. In our previous project, The Local Heroes, volunteers were involved from 58 cities from all states across India. Apart from paid memberships, we also have provisions for internships wherein students who are willing and motivated enough are provided with free of cost opportunities to gain experience letting aside their financial restrictions. In the upcoming years we also plan to expand our organisation and outreach to other countries and have started conversations regarding the same with people abroad.
The World Youth Heart Federation (WYHF) is a not for profit, registered as a section-8 company. We are a healthcare based non-government organisation providing services to improve the cardiovascular health of the society. The structure of the organisation consists of an Executive Board, Working Committees and Board of Advisors.
The Executive board includes the President along with Vice-Presidents for Internal Affairs, Finances, Networking, External Affairs and Public-relations, each with their well defined roles. The Working Committees on the other end go with the acronym of HEART namely Health education, Entrepreneurship, Advocacy, Research and Technology which take up different projects related to cardiovascular health independently or in unison.
The Health education committee works towards making health education videos for normal individuals, patients as well as healthcare professionals. These videos are made in multiple languages to improve outreach and include various training sessions, patient education material, disease and risk factor awareness etc. The Health Education committee also organises health-education webinars with special guest speakers and conducts quizzes for medical students. Currently they are working on videos related to CardioPulmonary Resuscitation (CPR) training modules and Hypertension awareness and home based blood pressure monitoring.
The Entrepreneurship committee works on setting up networks of mentors who can guide startups working towards cardiovascular healthcare. The committee also organises Hackathons in collaboration with incubators to give opportunities to young individuals in bringing effective cardiovascular health solutions.
The Advocacy committee works in two tiers, first towards raising awareness regarding various cardiovascular diseases via online and offline awareness campaigns and secondly they also work towards policy making in unison with the Research committee.
The Research committee primarily focuses on establishing multicentric research projects, which may be local or national via means of small working groups. They are currently working on a pan-India Hypertension research project along with various other smaller projects.
The Technology committee works in unison with the entrepreneurship committee in developing new technological advancements and indegenous healthcare solutions in the field of cardiovascular health.
- Individual consumers or stakeholders (B2C)
The World Youth Heart Federation India receives funding via various means but the most effective solution for self sustainability working for us is the ‘Hyper-Local Model’. through this model, our objective is to empower the local teams to look for funding options and raise donations locally to use those funds locally. This also serves an important concern of the donors regarding the usage of their funds making them assured that their philanthropic efforts were acknowledged. The donors see for themselves the changes brought about by their donations in their own surroundings which gives them a sense of security and develop increased interests in donations for the future as well. Another source of indirect funding for our cause which is similar to Hyper-Local model is the direct benefit to the beneficiaries by providing necessary requirements directly by the donors without any third party intervention but through the channel of WYHF. In some cases, funding from philanthropic donations are also used as seed funds for a working group until it becomes self sustainable.
We also plan to monetise the products of the Working Committees like training sessions of the Health education committee with a subscription based model for fund generation or monetary partnership with incubators and tech companies in collaboration with the entrepreneurship and technology committee or even possible monetization of potential and expensive research projects taken up by research committee etc.
Other sources of funding include crowdfunding collected via fundraising campaigns or membership fees which could be used for seed funding of various national and local projects and also help cover administrative expenses. One of the potential sources of funding also includes Corporate Social Responsibility (CSR) funds which could be used for large scale projects and also aid in long term sustainability. These funds are provided by profit making companies as a part of their social responsibility towards betterment of the community.