Climate Health Vulnerability Mapping
Geospatial analysis for communities vulnerable to climate related health impacts
Solution Pitch
The Problem
Climate Health Vulnerability Mapping (created by Khushi Baby), looks to address climate-related health outcomes such as: undernutrition, anemia, chronic lung disease, heat-related illnesses, vector-borne diseases, water-borne diseases, zoonoses, and mental health. The organization works primarily in Rajasthan, India where drought, heat-related illness, and lung-related deaths are of significant concern.
The Solution
Climate Health Vulnerability Mapping uses geospatial models to analyze the relationships between climatic factors and community health outcomes to plan data-driven public health interventions for the last-mile in India.
Stats
- 40 million beneficiaries have had their health tracked by community health workers using Khushi Baby’s digital health platform. These data points are used to inform climate health models.
Market Opportunity
Organization Highlights
- Climate Health Vulnerability Mapping by Khushi Baby provides digital health solutions to Departments of Health
Climate Health Vulnerability Mapping’s current partnerships include:
- Government of Rajasthan
- Government of Karnataka
- Research Partners: JPAL, Yale CarDS Lab, ARMMAN
AI/ML partners: Wadhwani Institute for Artificial Intelligence, Microsoft Research, Google Health, CMU AI Institute - Development Partners: JHPIEGO, UNICEF, UNFPA, WHO, PATH
Partnership Goals
Climate Health Vulnerability Mapping seeks:
- Collaboration with Geospatial Analysts specializing in climate and health modeling
Rajasthan, India's largest state and home to 80M people, is uniquely vulnerable to climate related health impacts. Over 2/3 of people live in rural regions, where in 90% of districts face severe water scarcity. Rajasthan is one of five states in India where India is facing record numbers of heat wavesrecord numbers of heat waves. Rajasthan's Bhiwadi industrial area was ranked worst city in the world for air quality, and Rajasthan has the highest burden of COPD and lung-related death in India. There are an estimated 300,000 brick kiln workers in Rajasthan who face the intersection of heat and air pollution related burdens. A study by CLRA found that over 90% of children of these families do not attend school. Rajasthan is also seeing an increase in vector and water-borne disease, further compounding already high IMR, MMR, non-communicable disease and malnutrition burden across the state.
We have developed a geospatial model to understand the intersection between climate related factors, social determinants of health, and health outcomes. These models identify areas where climate factors are disproportionately related to health outcomes. These visualizations are shared on a dashboard for health officials to plan focused interventions (screening camps, infrastructure strengthening, messaging campaigns). Models are derived from open source climate data sets and from Khushi Baby's Community Health Integrated Platform used by over 70K community health workers.
First map of Rajasthan's village-level multidimensional poverty index:
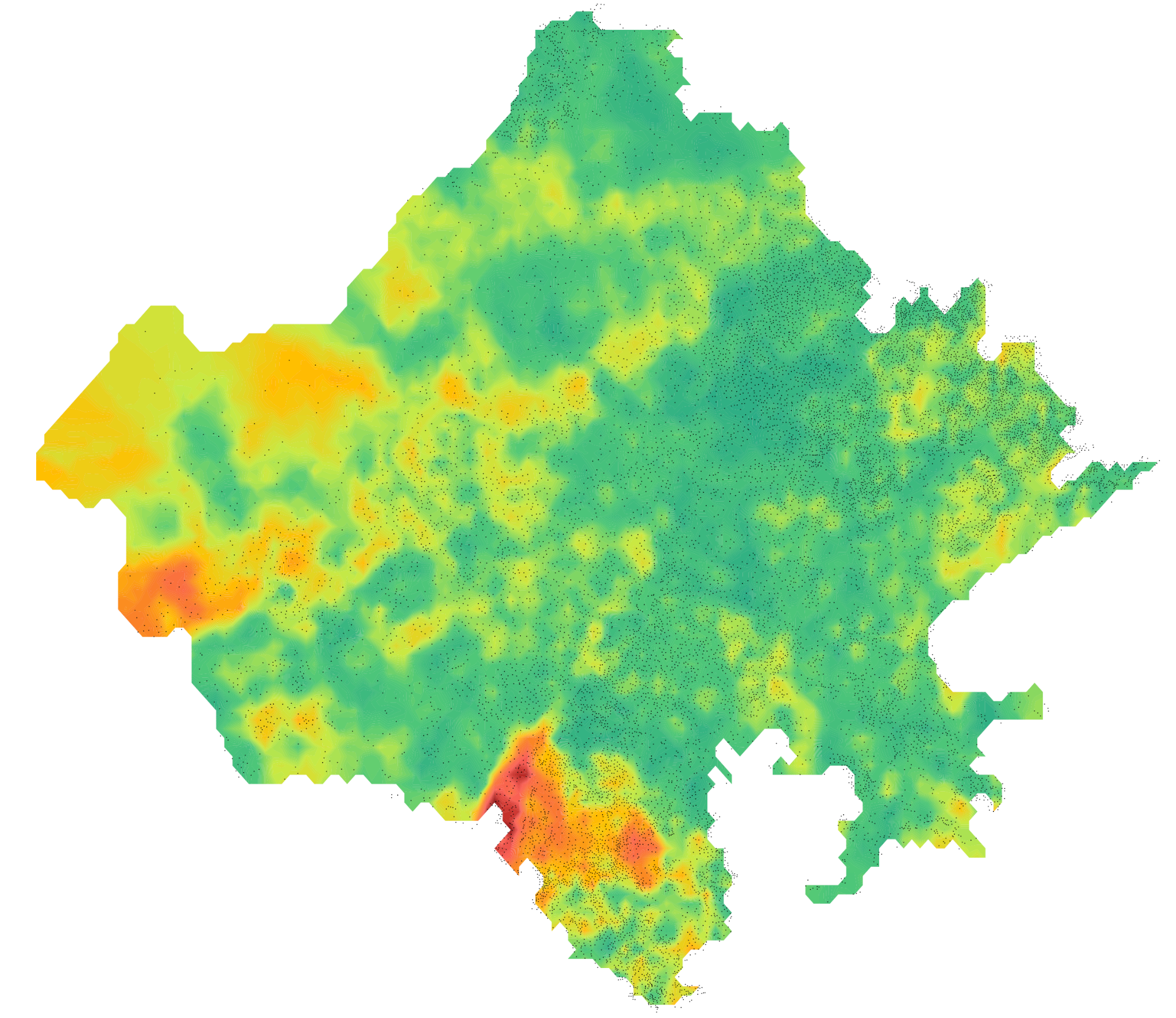
Our solution, the Community Health Integrated Platform and specifically dashboard, is designed for over 2500 health officials to use directly. The Community Health Integrated Platform applications is also used by 70K community health workers who can gain insights about climate-sensitive health factors in their own communities. Altogether the platform looks to drive data-driven engagements to improve the lives of over 40M people, whose health is currently tracked in the system.
The Khushi Baby team works as the nodal technical service partner to the Rajasthan's Department of Medical, Health, and Family Welfare. The solution - CHIP - is deployed at scale and has been used by 70K community health workers to track the health of ~40M beneficiaries. The solution is deployed by the Rajasthan Department of IT and is government owned. The Ministry of Health and Family Welfare has committed $13M for scale-up of the community health platform. Our team comprises of 65 interdisciplinary members spanning public health, medical, policy, field implementation and data science backgrounds and we work closely with state health officials.
- Enable informed interventions, investment, and decision-making by governments, local health systems, and aid groups
- India
- Scale: A sustainable enterprise working in several communities or countries that is focused on increased efficiency
40 million beneficiaries are tracked through the Community Health Integrated Platform currently.
We are looking to gain visibility, networking with a research community, build integrations with allied innovations, gain mentorship from domain experts, and also receive funding to support the integration of this new geospatial module within the CHIP platform.
- Financial (e.g. accounting practices, pitching to investors)
- Human Capital (e.g. sourcing talent, board development)
- Legal or Regulatory Matters
- Monitoring & Evaluation (e.g. collecting/using data, measuring impact)
- Product / Service Distribution (e.g. delivery, logistics, expanding client base)
- Public Relations (e.g. branding/marketing strategy, social and global media)
- Technology (e.g. software or hardware, web development/design)
CHIP has the largest geo-referenced, beneficiary-level health data set in Rajasthan with over 40M beneficiaries, with health outcomes across all major primary health verticals: RMNCH, non-communicable diseases, and communicable diseases. We are integrating this novel health outcomes data set with social determinants of health data also collected via CHIP and other open source geospatial models on climate related factors to understand areas of climate health vulnerability with up to village-level granularity for the first time in India.
We aim to integrate and deploy transformative geospatial models to identify climate vulnerable communities and guide data-driven public health interventions to impact the lives of up to 80M people living in India's largest state. We aim to share learnings from the Rajasthan Model to all of India and other LMICs with similar conditions.
- 1. No Poverty
- 2. Zero Hunger
- 3. Good Health and Well-being
- 5. Gender Equality
- 6. Clean Water and Sanitation
- 8. Decent Work and Economic Growth
- 10. Reduced Inequalities
- 13. Climate Action
- 17. Partnerships for the Goals
1. Scale CHIP to reach 60M people across Rajasthan (at least 75% of the health census of the state)
2. Scale CHIP dashboard to over 1000 weekly active users
3. Integrate geospatial models into the CHIP dashboard with village-level resolution
4. Implement automated impact evaluation feature in CHIP dashboard for local health interventions. Measure impact across 100 key performance indicators across health programs over time. Specific focus on child malnutrition, maternal anemia, mental health, heat-related illness, vector-borne disease, heart disease, and COPD.
Community Health workers use the CHIP platform to collect social determinants of health including environmental exposures, health behaviors, and health conditions in a village-level health census.
Health officials use the CHIP dashboard to understand climate vulnerable communities and schedule data-driven interventions (local health camps for screening, messaging campaigns for health behaviors, infrastructure strengthening projects, and human resource allocations).
Beneficiaries receive CHIP-platform generated awareness messages to improve their climate resiliency. Community health workers receive due-lists of beneficiaries and micro-communities which are climate vulnerable.
Community health workers save time from manual reporting (up to 20 hours a month) and receive higher and on-time payment for activities performed, making space for improved counseling and travel to hard-to-reach communities in climate vulnerable zones.
Empowerment of the community health worker (digital, clinical, and financial), health official (digital and public health planning), and beneficiary (public health awareness) drives improved demand for primary health services, improved primary health service delivery, resulting in improved screenings of climate-sensitive disease, improved completion of referrals at primary health centers, and improved treatment of climate-focused diseases (malnutrition, anemia, heat-related illness, vector-borne disease, heart disease, lung disease, mental health).
Community health workers use an android application. Health officials use a web application. The platform analytics leverage geospatial modeling and machine learning technologies.
- A new application of an existing technology
- Artificial Intelligence / Machine Learning
- Big Data
- GIS and Geospatial Technology
- Imaging and Sensor Technology
- Software and Mobile Applications
- India
- India
- Nonprofit
We have an interdisciplinary team of 65 full time members, including public health practitioners, designers, communication experts, field monitors, data engineers, data scientists, android developers, backend developers, testers, and health care providers.
99% of the team members live in the LMIC / country where the solution is deployed and are people of color. We are working to improve gender balance within our team.
We have spent over 180K hours co-creating our solutions with community health worker partners in the field.
We raise funds from iNGOs, family foundations, CSRs, and awards. These funds support the services we provide to governments free-of-cost. The government then leverages our services and adopts our solution to create impact at scale. Our donors ask us to report the impact and essentially fund for impact created.
We also engage in contract based work with development partners, who look to leverage customized versions of our solutions in geographies where our teams have a mutual presence and government alignment.
- Government (B2G)
1. Improve scalability and interoperability of CHIP platform by alignment with DIIG principles and ABDM certification to expand access to Digital Square donor base and further government-funded RFPs in India.
2. Build in-house resource mobilization unit and expand in-house monitoring and evaluation team for identification and donor relationship as well as improved impact reporting
3. Raise funds from multi-year, catalytic grants from iNGOs / family foundations in the Data Science for Good and Digital Health spaces
4. Raise at least 20% of revenue from contract-based work with development partners such as JHPIEGO, JSI, PATH, WHO, UNICEF, UNFPA, etc.
5. Develop pipeline for research-based funding through creation of synthetic public health research databank, whereby research efforts could be cross-applied to original data without exposure of original data
We have received about $3M in funding to date, for a community health worker digital health platform that has reached 40M beneficiaries and 70K health workers. Compared to others in the space like Medic, we are operating at 15x less cost / beneficiary, with double the number of beneficiaries reached. Our platform has also been supported through Government of India investment of $13M (although that funding does not support our direct services).
We are looking to sustainably grow our team by building a diverse source of revenue streams across family foundations (e.g. PJMF), iNGOs (e.g. GAVI), CSRs (e.g. ARM, Google.org) who are looking to make investments in longer-term digital health strategy for LMICs.
Organization Type:
Nonprofit
Headquarters:
Rajasthan, India
Stage:
Scale
Working In:
India
Current Employees:
65
Solution Website:
https://play.google.com/store/apps/details?id=org.khushibaby.ashadh
Solution Socials:
Twitter
Instagram
LinkedIn

Strategy and Research Lead

COO

Lead - Development