MammaCare Global Breast Exam Network
Women in affluent countries benefit from well funded breast cancer early detection infrastructure resulting in a five-year breast cancer survival rate of 85-90%. In Sub-Saharan Africa (SSA) fewer than half <50% of the women with breast cancer survive beyond five years and this disparity increases further for young women in LMICs.
Importantly, women of childrearing age in LMICs suffer from endemic, late stage breast cancer with devastating personal, familial and social hardships. Poor survival from breast cancer among young mothers in African LMICs invokes urgent concern over the expanding intergenerational impact of maternally orphaned children.
Of all presenting symptoms, the probability of breast cancer increases 10 fold when a lump is present. Although physical, clinical examination of the breast (CBE) is considered the most affordable intervention for detection of early breast cancer in LMICs, its common practice is variable and deficient, lacking standards of performance and accuracy. These limitations undermine the effectiveness of breast exams performed by primary LMIC providers minimizing their global impact.
It is widely acknowledged that the earliest and most common symptom of breast cancer is a lump, detected by hand. Among the scientific and clinical reports on the subject, a 2015 landmark review by The International Agency for Research on Cancer, (IARC) in the New England Journal of Medicine concluded that improving and expanding clinical breast exams (CBEs) in LMICs will lower the stage of breast cancer when first detected so that it can be effectively treated. In response, our team of university scientists and clinicians created and published the first experimental technology to measure and valdate the tactile sensory and motor skills that are required for accurate and reliable detection of the earliest stages of breast cancer. The project, originally funded and named Mammatech, became MammaCare.
With the support of the National Science Foundation we created the first computer-guided hands-on breast exam trainer whose technology compares exams performed on the trainer by users to built-in standards of accuracy and thoroughness. A series of modules provides real-time feedback that shapes exam performance until rigorous standards of accuracy are achieved and verified. The resulting skills are practiced to reduce fatal delays in detection. The team formed the MammaCare Foundation (MammaCare) to deploy the technology and in 2021 and 2022 extended the network to Ghana and Haiti to provide computer guided training via a low-bandwidth training network for local primary providers. Data analytics from network trainees in Africa and Haiti verify acquisition of the essential skills required to conduct quality-standard breast exams within their communities.
The MammaCare CBE Simulator is a web-based, self-administered training platform that now operates over a browser to teach and measure the user’s breast exam skills and progress in real time with continuous feedback. Within 2-3 hours of instruction and hands-on practice, the system quantifies performance, corrects examination deficiencies and validates user competencies for the trainee and/or supervisory staff. Primary providers learn to reliably detect multiple suspicious masses (0.3cm - 1.0cm) without increasing false positives.
Nurse Confirming Detection of Suspicious Lump During a Breast Exam

Size of Tumor by method

Continuous Feedback During Training (true positive detection)

Continuous Feedback During Training (false positive detection)

Exam Performance Feedback (final exam appears when standards are met)

Summary: Tumors Detected, Tumor Sizes, Exam Duration, %Tissue Coverage
Local computer minimum specifications: OS: Any RAM: 2gb Software: Google Chrome browser Hardware: 1x 3.0 USB port Min. internet speed (down/up): 3/1 Mbps If internet connection is lost during a clinical breast exam assessment, the performance results can be saved on the local HDD and uploaded when the internet connection is restored.
Women in LMICs suffer disproportionately from loss of productive life
years due to the disabling impact of late-stage breast cancer, a
disparity that is expected to increase for the next two decades.
The burden of late-stage breast cancer is calculated in terms of the number of disability-adjusted life years (DALYS) and years of life lost (YLLs). In 2017 alone, women in LMICs collectively lost 18 million years of productive life from advanced breast cancer detected at late stages.
Over the last two decades, high income countries have experienced a steady decline in early mortality among young women, <50 years old. During the same period among LMICs, particularly in Africa, there is a steady increase in late-stage breast cancer and mortality among younger women between 30 and 45 years of age. "Age-wise, breast cancer incidence [and mortality] increased [in younger women] up to the 45–49 age-group and declined after that. This pattern was repeated in nearly all African countries, with the incidence [and mortality] being the highest in young to middle age-groups (30–50) [years old] "

According to public health authority Subhojit Dey, MBBS, MD(AM), MPH, PhD, developing a global corps of trained, frontline clinical breast examiners is the most effective approach to prevent the late, devastating physical and socioeconomic consequences of the disease in LMICs.
In July 2021, our team successfully deployed the clinical breast exam training technology to primary care clinics in the following Ghanaian cities: Kumasi, Mankessim, Adenta, Kasoa and Cape Coast. The original clinical breast exam training protocol was further developed with the collaborative support from local Ghanaian clinicians that examine women in their communities. All training materials were reviewed by local clinical leaders for cultural relevance and appropriateness.
The lessons learned from this pilot program have established a strong foundation for scaling up to a national training program throughout Ghana and other LMICs that will benefit.
- Employ unconventional or proxy data sources to inform primary health care performance improvement
- Provide improved measurement methods that are low cost, fit-for-purpose, shareable across information systems, and streamlined for data collectors
- Leverage existing systems, networks, and workflows to streamline the collection and interpretation of data to support meaningful use of primary health care data
- Provide actionable, accountable, and accessible insights for health care providers, administrators, and/or funders that can be used to optimize the performance of primary health care
- Balance the opportunity for frontline health workers to participate in performance improvement efforts with their primary responsibility as care providers
- Growth
Advances in technology have enabled us to rapidly improve the effectiveness of primary providers at little cost, globally. Nevertheless, severely limited resources in LMICs inhibit training the hands of practitioners in LMICs who would benefit most. This Challenge, if awarded, will directly reduce that barrier because the resources provided will be used to advance training where it is most urgently needed.
We currently provide the training platform, a Palpation Assessment Device [P.A.D.], four tactually accurate breast models synchronized to the training protocol) and interactive coursewear at or below our internal costs to deploy training as widely as possible. We apply a small annual fee to support the server and data management costs for each breast exam trainer.
With the grant from this Challenge, we can deliver essential training to an expanded corps of LMIC primary providers who could not otherwise obtain or afford it. There are many deployment strategies that will make large-scale, countrywide training sustainable and cost-effective. Ample evidence supportsthe provision of verifiable breast exam skills as the first step in reversing the negative health and socioeconomic burden of late-stage breast cancer that millions of women currently endure.
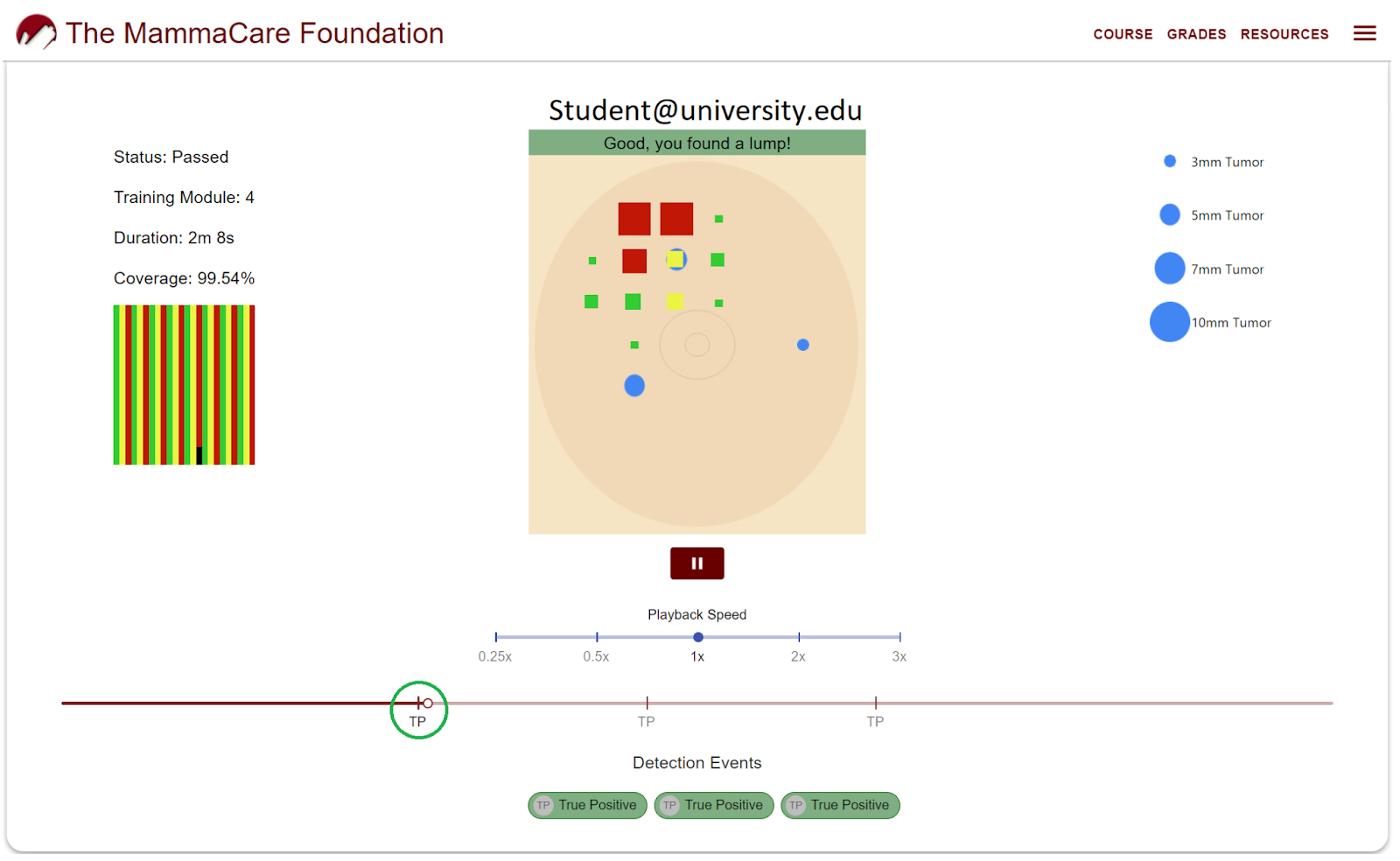
In practice the training platform monitors progress and generates data analytics directly from the hands of the user. The results below are from an exam performance on one of four training modules. Result shows progress on three key measures left to right: tumors detected and missed, location, pressures applied (depth of palpation), percent of tissues examined/unexamined, pattern and duration of exam.
The nearly universal favorable response to post training questions from nurses, midwives, primary practitioners and students reveals significant positive increases in self-reported confidence and self-perceived competence in performing breast exams.


To our knowledge, this is the first complete technology that can capture and replicate digitally, the sensations produced by mechanoreceptors in human fingers during palpation of an organ, manage the data stream generated during the exploratory exam, analyze learning progress, detect errors and stream corrective practice to the user in real time via a browser connected device to cloud-based software. Moreover, to our knowledge there is no other technology that can compute a user's tactile sensation and confirmation of small suspicious tumors.
Importantly, we know that humans possess an exquisite multi-layer tactile sensory system that improves with training and experience while practicing on musical instruments, while learning to "reading" Braille dots with fingers, and in everyday tactile learning and mistakes such as detecting the softness of a tomato before purchase at the market or the hardness of apples or the variations in 5 grades of fine sandpaper. These examples of tactile sensory events suggest that learning, skills acquisition progresses with practice, or musicians would not improve, and we would purchase nearly rotten tomatoes
Like all sensory learning, breast exam competencies increase with practice involving both motor and tactile skills. To elevate breast exams to measurable standards of performance, we took advantage of highly sensitive sensory electronics, advanced materials, cloud-based data analytics and networking that now mirrors and connects directly to the sensations in examining fingers teaching them to reliably discriminate between normal complex breast tissues and suspicious sub-centimeter breast tumors, a technology we developed for early detection of breast cancer, where it is needed most.
Our goal for the next 12 months is to steadily increase training frontline providers in Ghana and Haiti enabling them to reach a meaningful proportion of women at risk in their care. Data from our pilot studies in these countries as well as from our domestic network, suggest that within five years we can reasonably project, based on a sufficient number of connected computer guided trainers (~1000 ), that at least one million at risk women of child reading age within a national population of 16 million women will receive annual, quality standard breast exams. Equally important, once the corps of trained practitioners is in place, women who self-examine and/or adventitiously detect a suspicious change will have immediate access to a competent examiner who is capable of confirming and following up the woman's self-detected lump or symptom.
The direct effect of computer guided breast exam training on pracitioners skills is determined in two ways: digitally, through automatic data analytics that calculate each examiners (users) pre-training and post-training accuracy (sensitivity specificity and thoroughness). The users self-reported confidence and competence of users is also obtained using a likert scale evaluations and open comments to determine the perceived value of training. Naturally, the longer range and most important effect is the impact on women's health and survival and this analysis is the subject of a multi-year study that is underway.
Independent review and research indicate that clinical breast exams require special standards and skills to measurably and uniformly improve breast cancer examination practices that can advance early detection. There is good evidence that late stage breast cancer in LMICs can be downstaged with the subject, standardized computer guided breast exam training technology if and when deployed among frontline workers in LMICs.
The direct and neural effect of skill training on human performance and cognition are well presented in this report, which best explains the biobehavioral processes involved in acquisition and performance of skilled tasks.
Please refer to the earlier descripitons of the science and engineering behind the technology and its application and effect on the skills and performance of breast exams.
- A new technology
- Behavioral Technology
- Biotechnology / Bioengineering
- Imaging and Sensor Technology
- Manufacturing Technology
- Software and Mobile Applications
- 3. Good Health and Well-being
- Germany
- Ghana
- Haiti
- United States
- Germany
- Ghana
- Haiti
- United States
The data from learning, practice and completion of the training protocol are automatically generated and analyzed. Certificates of completion and/or continuing education credits are made available where possible to reward completion.
- Nonprofit
- Organizations (B2B)
MammaCare Foundation clients provide a revenue stream that supports our operations. In addition the foundation seeks and receives grants to advance and deploy breast cancer training technologies

Sr. Reseach Scientist and Chair, Mammacare Foundation