Medupi Rapid TB Diagnosis Tool
Tuberculosis (TB) is the second leading cause of death from a single infectious agent, after COVID-19. In 2020, TB infected more than 10 million people and claimed 1.5 million lives. At least 86% of the world’s TB burden comes from 30 high burden countries, of which 22 of them are low-and-middle income countries (LMICs).
The most widely used test for diagnosing TB (with more than 77.6 million tests performed each year) is Sputum Smear Microscopy (SSM). Despite having the lowest performance amongst all the diagnostic tests (sensitivity of ~50%), it is still the most preferred test, costing about $1.
In recent years, Nucleic Acid Amplification Tests (NAAT), such as GeneXpert, have been introduced to National TB programs. Despite WHO recommendation and increased funding, the uptake and accessibility of these tests has been low. This is because these machines ($30k) and assays are high cost (~$15/test) and require sophisticated infrastructure (such as reliable electricity, air conditioning, constant water supply etc.) that is simply not available at the primary health centers (PHC) where TB patients access the system. In India, for example, NAAT based tests are limited to tertiary health centers, inaccessible to patients in terms of (1)location - these centers are based in cities (a city will have only 1 or 2 of these high cost systems) and, (2)patients typically have to be referred from a primary health center, before getting a NAAT test at the district level facilities (in villages, patients will typically go through village centers and subcenters, before reaching primary health centers where they can access sputum smear microscopy if so deemed).
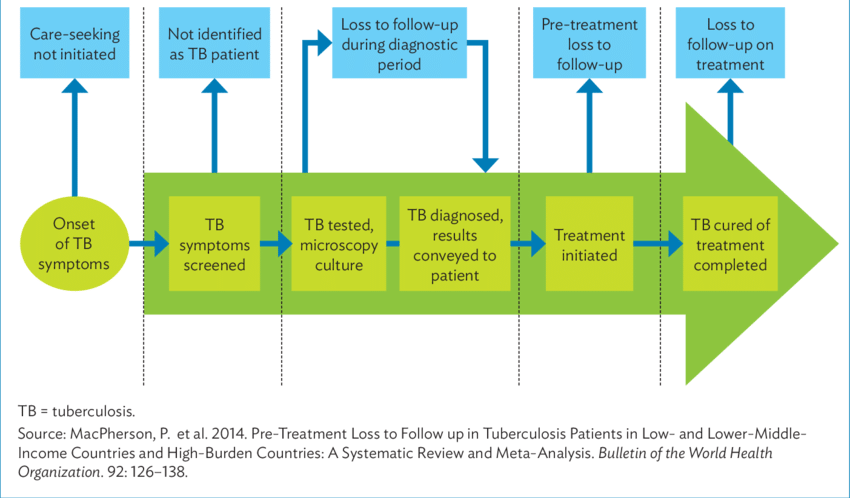
From the patient's perspective (especially in populations who have to make a choice between missing work that brings food for the day or week), when symptoms first appear they neglect them or self treat (home remedies or local pharmacies). They may then present at village centers/subcenters where they can be misdiagnosed (treated with broadspectrum antibiotics). If suspected, they may be sent to a TB clinic where their sputum is collected. They have return the next day to collect results, submit another sample, and may be referred to a pathology lab or hospital for a chest X-Ray.
From onset of symptoms to initiation of treatment can take upto 4 months, depending on where you live and your economic status. During this time, your condition goes from bad to worse, your ability to work suffers. This often has huge financial implications. During this time, you infect 4 other people in the community, who will also be months away from being discovered. TB, in effect, will become a community's problem.
There is a need for tests that are cheap enough to enable governments to actively over-test in communities, fast (returns results in minutes, not hours or days) enough for presenting patients to get initiated on treatment at an early stage, portable enough to be placed at every point in the healthcare system, and easy-to-use enough to be administered by minimally trained health workers.
Community Care Workers (CCWs), for example, decentralize TB services by reaching patients at both PHC clinics and at their homes. CCWs in India, for example, routinely cover a hundred people each day. A device in hands of CCWs, will enable TB programs to move at the pace of the disease and its transmission. It'll enable real-time surveillance, surgical surge of resources, localized quarantines and care in communities often left out of the system.
Medupi is a low cost optical TB testing system, designed to work within existing national TB program guidelines, for active screening of suspect TB patients in their homes, or presenting at primary clinics.
The Medupi rapid diagnostic tool, has two main components:
Cartridge
The cartridge is a disposable plastic piece that looks like a microscope slide. It contains a polymer based microfluidic mechanism that concentrates TB causing mycobacteria from patient's sputum sample to a small spot on the cartridge. This isolates TB bacteria from other organisms found in sputum samples, resulting in a high performing sample to be tested.
Since most national TB programs are still heavily reliant on microscopy (in India, for example, 8.2 million microscopy tests were done compared to 2.3 million NAAT tests), the cartridge has been designed to work with both microscopy and our Medupi reader system. The use of Medupi cartridge increases the sensitivity of microscopy from 50% to over 90% and reducing the limit of detection from 10,000 CFU/ml to 500 CFU/ml - this alone can positively affect about 4 million test results in just India.
2. Reader system
The reader system is a briefcase sized optical system, designed to read optical signatures from the cartridge (Our current prototype is electrically powered and has not been optimized for size - we plan to easily reduce the size of a laptop by production phase)
It uses proprietary optical scattering measurement systems and algorithms to identify unique signatures of TB mycobacteria. The data collection, analysis, and results reporting is automated, thus, requiring minimum handling by health workers. The Medupi reader has an expanding library of signatures - we envision this will help us create a system to deliver last mile diagnostics, not just for TB but for other high priority diseases in the future.

Our plan is to push roll-out starting with India. India has the world’s highest TB burden, and the Indian government has set and is actively pursuing, an ambitious goal to make India TB-free by 2025. This is ahead of the United Nations’ Sustainable Development Goal (SDG Target 3.3) of eradicating TB from the world by 2030. Our target populations include
1. Homeless populations (while we're starting with India, we see this as an important population in even developed nations, such as the US - People expressing homelessness (PEH) are 4 times as likely as the overall population to have TB)
2. Urban Slums (These include migrating workers, factory workers and construction workers; Overlap with labor force populations)
3. Labor force populations (studies have shown occupations of being the labor force as strong predictors of delayed care seeking behavior. Instant testing and immediate enrollment into treatment is extremely important for this population)
4. People living with HIV (including sex workers - having a low limit of detection is very important for these populations since their TB bacteria load is generally low)
5. Rural (including those in tribal communities accessing healthcare through government and NGO initiatives. Many in the rural population live in hard to reach areas, but have similar outlook of self medication and delayed care seeking behavior as other populations - it is imperative that they can be reached in their own homes, tested and initiated on treatment if necessary, without having for health workers to comeback)
Our team has existing partnerships with study partners (YRG Chennai is helping conduct our field trial in India and we also have written directive from the Health Secretary in Rajasthan towards conducting studies at the Institute of Respiratory Diseases, Jaipur), non-profit organizations, universities in India and is looking to collaborate with organizations to understand most effective placement and use cases, try demonstrations of effectiveness with CCWs, conduct user research. There has been a lot of written interest In initial meetings with state health officials (State of Rajasthan) as well as health agencies (ICMR) in India, and we're looking to find partners and community who can help bring this to officials and agencies supporting eradication of TB around the world.
We plan to expand future field studies to South Africa, as we continue to engage with our in-country partners in the iterative design process of Medupi.

Drizzle Health's core team is composed of I (Bonolo Mathekga) and Digvijay Singh. Me and Digvijay were born and raised in South Africa, and India respectively. We have been personally affected by the plight of TB in our home countries in various ways. This has been the primary force driving us to work on developing solutions to address TB, from the onset of our careers. We have firsthand experiences working with CCWs on the ground in South Africa, and India, as they go door-to-door providing TB services to their communities. We have collectively spent over 200 hours conducting stakeholder interviews with CCWs, community leaders, government officials, doctors, nurses, TB patients and their families. Throughout all of these experiences, we have grown to have a deep appreciation for the work that CCWs do, not only for TB, but for HIV/AIDS, as well as non-communicable diseases too. CCWs are the unspoken heroes of healthcare systems in LMICs. Digvijay and I feel passionate about creating technologies that will help make them more effective at the very important work that they do.
Throughout our design process, we have held numerous design sprints, ideation sessions and co-creation sessions with different stakeholders involved in the TB care pathway, right from CCWs to epidemiologists. We are also constantly engaging with our partners in India, South Africa and the US, to get feedback on our design process. We're currently working towards hosting a virtual listening session with CCWs, TB patients, and researchers in South Africa to learn how reimbursement for CCWs works, as well as how the on-going Covid-19 pandemic is affecting active TB case finding at a community level.
I went to the University of Witwatersrand in South Africa where I got my bachelors in Information Engineering, and Biomedical Engineering. Digvijay studied Materials Science at the Indian Institute of Technology, Varanasi and worked in product design and ethnographic research for a few years. We met at the Johns Hopkins Center for Bioengineering Innovation and Design where we did our masters. Over the last 3 years, we as a 2-person team (with our mentors, collaborators, interns and contractors) have managed the R&D, as well as testing and fundraising requirements of the project. We're supported by mentors from the Johns Hopkins University with extensive backgrounds in global health and infectious disease research, cutting-edge nanomaterials research as well as TB, mycobacteria and epidemiology. Our other mentors are experienced in production, TB testing in primary and tertiary clinics, treatment of TB in communities, regulatory and state health machinery.
Through personal, professional and academic connections, we have been able to reach a variety of stakeholders, experts and mentors. There are, also, gaps in the types of stakeholders and expertise. These have included grant writing/global funding experts, production engineering experts, key opinion leaders in various communities, fundraising experts, specific target populations, etc. We anticipate that our team composition will evolve over time to reflect our learnings and engagement with target populations as well as our requirements for development and implementation; but this is a process we hope to accelerate through our involvement with the MIT Solve community.
- Build fundamental, resilient, and people-centered health infrastructure that makes essential services, equipment, and medicines more accessible and affordable for communities that are currently underserved;
- Pilot
As we complete our transition from research and design to the engineering and production phase of the project, we're looking for mentorship, partnerships, funding and hiring for our company. Major areas of support for us are:
1. Partners for field trials - We're currently on our way to conduct field trials in India but have been dependent on a single partner (leading to delays and limits of study). We're looking to engage with partners who can use our devices in their projects and settings and not only help create field data, but also iterative design changes based on specific population feedback. We're also looking for partners who's work is specifically geared towards our target populations.
2. Partners for research - We're also looking for partners working in research settings, especially studying diseases in underserved populations towards creation of data for recognition through the reader in similar ways (We're currently also working with the Sexually Transmitted Diseases group at Johns Hopkins on this).
3. Funding - We're in the detailed engineering phase for our cartridges and at the design freeze phase for our reader - we're looking to scale up prototype production. We're also looking to hire engineers, a grants person and a regulatory consultant. We have access to experts in some of these areas but will be looking to on board people in a part-time/full time capacity. We're also looking to reimburse and pay for larger field studies beyond our upcoming one.
4. Personnel - As mentioned, we're looking to hire great people who also strongly believe in our mission - engineers in materials, optics, electronics and production/manufacturing to support engineering requirements of the project, a grants person and a regulatory consultant. We currently have some HR and Legal support that we will be able to expand when we have more people.
5. Mentorship - Navigating fundraising, approvals through governments and official bodies, and expanding our network to include more buy-in from the customer.
Being a part of the Solver community will provide us with the opportunity to refine the way in which we tell our story. This is imperative to our growth as a startup, as we work towards attracting new investors, collaborators and other key players whose contribution is pivotal to moving us closer to our next goal post.
The mentorship, strategic advice, and coaching sessions will add value to our venture, by providing regular objective feedback. Moreover, being a part of an environment that fosters creativity and growth, is invaluable to us as individuals, and even more so as a team.
- Monitoring & Evaluation (e.g. collecting/using data, measuring impact)
Imagine being in the battlefield. Would you want to act based on information that is weeks old or minutes old? TB and its transmission are currently outpacing current approaches. By the time, objectively ingenious plans are executed, the battlefield changes (people move around, come in contact with other people, travel and spread TB in unpredictable areas, undetected), reducing the effectiveness of those plans.
Our solution is unique in that it is a proactive test that can move along with TB transmission at a community level. Our device makes use of infrastructure that already exists at primary clinics where the majority of patients first interact with the public health system. Furthermore, our solution is powerful in that it can enable CCWs and health practitioners to be more effective at doing active case finding door-to-door, area-to-area and contact tracing in their communities. And in doing so, reuniting patients with their results within the same visit of collecting their sputum samples, and initiating treatment right there and then. This extremely fast turnaround can help governments sweep entire communities very quickly, put local micro-quarantines and provide support resources with precision. This can only be enabled if testing is low cost enough, returns results fast enough, can be mobile and used with minimal training.

Now, there are some engineering features that we're still working on. But our approach and device design paves way for the agility and interoperability needed to stop these vicious hidden cycles of community spread that often have devastating effects on the health, finances and humanity of people and families, and ultimately communities.
We believe that this model will ultimately be able to support other community based diseases, using research and data from other groups and organizations in the field - In the long run, we envision strong local ecosystems for the community and by the community (which is pretty different from the centralized facility approach in the developed nations dictated by state-of-the-art high cost machines).
Short-term (first 2 years, since we need to await approval post testing) - (Through Cartridge sales only)
- Increase number of bacteriologically confirmed TB cases
- Increase TB notification rates
- Patients get correctly diagnosed the first time
- Ease of accessibility encourages more people to get tested
- Reunite patients with their test results
- Initiate patients on TB treatment
Long-term (2-5 years) (Use of the complete Medupi system)
- Any presumptive TB patients, if they access public healthcare, will get correctly diagnosed, creating a positive impression of the system and process
- Decrease TB incidence rates and deaths
- Increased population covered in active tracing efforts
- Reduction in number of hidden TB patients
- An easily accessible, accurate and fast test encourages more people to get tested
- Doctors’ distrust on utility of point of care tests for TB is reduced
- Increases quality of life amongst afflicted population
- Reduce TB stigma due to faster relief from signs and symptoms
- Reduced incidence rate of multi/extreme-drug resistant TB (due to improved monitoring of active TB cases)
- Establish TB outbreak surveillance
We will achieve our impact goals by using our products to test presumptive TB patients at point of care settings. We will work alongside CCWs, and lab technicians to conduct TB testing and report the results to both the patients and the national TB registry in a timely manner.

We currently have partners in place to produce our beta prototypes of our cartridges (in thousands). As we finish our detailed engineering phase for our cartridges soon, we will be working with our existing partners and also looking for new partners towards higher production numbers in hundreds of thousands (we already have quotations for these).
We are looking for partners and organizations that have gone through the process of mass manufacturing complex electronic products - While we currently have a BOM based on high level designs from vendors, we're looking for support in planning and manufacturing for our Medupi reader while it undergoes a detailed engineering phase.
As shown in the timeline above, we will begin with small pilots of the cartridge in 2 states (Uttar Pradesh and Rajasthan) - While we work through the state health departments, we are also looking for partners already working with target populations in these states. We will then expand our program in the states over the next year until approval for our reader system. Post that, we will both, work with partners and directly with state health departments for roll-outs within state health infrastructure.
We are working towards the UN's SDG Target 3.3 of ending the TB epidemic by 2030. Progress made towards achieving this goal will be measured by monitoring the reported TB incidence rates (called TB notification coverage in India) , following the implementation of our technology. Additionally, the number of bacteriologically confirmed TB cases, and the number of patients that are initiated on anti-TB drugs are all key performance indicators which we will be closely monitoring.
Our product is ultimately expected to have an impact on contributing towards making India TB-free by 2025. This will be achieved through a series of short and long term outputs shown below.

A multifaceted approach is required to eradicate TB, because testing alone will not address all the complexities of the disease. Improved anti-TB drugs, treatment of the pool of latent TB infected people, the development of a TB vaccine, and non-health interventions are some of the critical activities required to win the fight against TB.
According to the National Strategic Plan To End TB in India 2020-25, a 25% increase in active TB case finding by 2025 will decrease the TB incidence rate to 170 cases per 100 000 population. While, a 30%, 70%, or 90% increase in active TB case finding will result in a TB incidence rate of 148, 120, 44 cases per 100 000 population respectively [1].
For example, Rajasthan (where we have existing partnerships) has an estimated population of 81.2 million people and accounts for ~7% of the total TB burden in India [2]. Currently, 89% of bacteriologically confirmed TB cases are performed using SSM, X-rays, and TB culture [2]. With our technology being used to replace only 30% of the tests performed at PHCs, we could correctly diagnose an estimated 44 954 TB patients in our first year of operation alone.
[1] National Tuberculosis Elimination Programme, Ministry of Health and Family Welfare (2020). National Strategic Plan To End TB in India 2020-25
[2] Central TB Division, Ministry of Health and Family Welfare (2022). India TB Report 2022: Coming Together to End TB Altogether. https://tbcindia.gov.in/
The cartridge is powered by our polymer system that concentrates TB causing bacteria to one spot. The TB-capturing cationic polymer system, poly diallyldimethylammonium chloride (pDADMAC) has previously been shown to have a high affinity for mycobacterium [1-4]. Non-provisional patent in both the U.S., and India have been filed.
The reader makes use of a polarization imaging technique to probe the microstructural and optical information of TB bacterial colonies [5]. The system is composed of an optical light transmitter and receiver, which detect the presence of a unique TB signature on the cartridge. Optical signals are then processed and analyzed by comparing it to an existing library of bacterial signatures, thus leading to a positive or negative TB test result. Non-provisional patents are currently under processing.
[1] Albert H, Ademun PJ, Lukyamuzi G, et al. Feasibility of magnetic bead technology for concentration of mycobacteria in sputum prior to fluorescence microscopy. BMC infectious diseases
2011;11:125.
[2] Liu J, Sun ZQ, Pei H, et al. Increased case finding of tuberculosis from sputum and sputum deposits after magnetic bead concentration of mycobacteria. Journal of microbiological methods
2013;93:144-7.
[3] Wilson S, Lane A, Rosedale R, Stanley C. Concentration of Mycobacterium tuberculosis from sputum using ligand-coated magnetic beads. Int J Tuberc Lung Dis 2010;14:1164-8.
[4] Tadesse M, Aragaw D, Rigouts L, Abebe G. Increased detection of smear-negative pulmonary tuberculosis by GeneXpert MTB/RIF(R) assay after bleach concentration. International journal of mycobacteriology 2016;5:211-8.
[5] Badieyan, Saeedesadat, et al. "Detection and discrimination of bacterial colonies with Mueller matrix imaging." Scientific reports 8.1 (2018): 1-10.
- A new application of an existing technology
- Biotechnology / Bioengineering
- Imaging and Sensor Technology
- Materials Science
- Software and Mobile Applications
- 3. Good Health and Well-being
- India
- South Africa
- For-profit, including B-Corp or similar models
As a team, we firmly believe in acknowledging our differences in race, color, sexual orientation, gender identity, religion, disability, age, genetic information, veteran status, ancestry, and national or ethnic origin. It is only by acknowledging what makes us different, that we are able to truly embrace and celebrate our diversity. These differences govern how we uniquely experience the world, and motivate our decisions on when and how we access healthcare, the type of diseases endemic in our communities, and the medications available to us.
Our goal is to fight TB and the destruction it is causing millions of lives around the globe each year. We understand that this is a fight where we need all the help we can get and need to rely on the best of each other.
The team's co-founders have differing backgrounds. Digvijay is an Indian national, hailing from the national capital region. Bonolo is South African and named the product Medupi, a Sepedi word that means gentle rain. Medupi is considered a blessing, as it is pleasant rain that soaks parched land, yielding a plentiful harvest. This aligns well with what we imagine equitable healthcare to look like. Rain affects everyone, regardless of socio-economic status, cultural, and identity-based human attributes. Similarly, our goal is to make healthcare accessible to everyone, regardless of socio-economic status, cultural, and identity-based human attributes.
This spirit is reflected in our current team and extended team, and will guide us as we expand.
Our primary business model is simple: Charge per device and cartridge.
We plan to sell each cartridge for $1-1.5 (NAAT based systems require cartridges costing around $15 each). Our proposed price point falls well within guidelines set by the Foundation for Innovative New Diagnostics (FIND) and the World Health Organization's (WHO) Target Product Profiles. At scale, BOM for cartridge fall under $0.25.
We plan to sell each device for $3000-5000 (awaiting pricing interviews with stakeholders). At scale, BOM for the reader fall under $1000.
For the purposes of our 1-3 year plan, our customer is the Government(s) of India (states and ultimately center). The central government has declared that they'll make the country TB-Free by 2025 - There's political capital attached to the massive goal. This is an urgent problem for them. Diagnostics is a huge part of that problem. And there's a lot of initiatives and finances that have been set in motion to achieve that goal.

(Source: National Strategic Plan to End TB in India 2020; Scenario SDG denotes scenario for achieving TB free country)
The National Strategic Plan to End TB in India 2020 report shows that according to the government's own estimations, India will need to conduct 6 times more tests. And over 90% of the population will have to be screened.10 million tests were conducted in India last year. To do these tests using NAAT for 5 years would cost $750M. To test at the rate India would need to, would cost $4.5B. Our initial target states (where health officials have expressed a lot of interest in our products) of Rajasthan and Uttar Pradesh, the expenditure was $7.8M and $4.8M on diagnostics alone. To attain SDG scenarios, these would be $240M and $150M over 5 years. Needless to say, for a lot of governments, such high numbers are unsustainable without foreign aid.
Using our device, in an ideal world, India's 5 year cost would be $300M. These huge savings would allow the government to not only increase funding for treatment, but also:
1. Test all people presenting with symptoms
2. Test contacts of people presenting with symptoms (contact tracing)
3. Conduct door-to-door screening, impose 'mini-quarantines' based on instantaneous (not weeks old data) (active case finding)
4. Monitor treatment of patients initiated on treatment and track drug-resistant cases.
This can only be possible due to low device and per test costs, AND almost immediate results.

This graph shows the impact of using Medupi on a large scale in our initial target states of Uttar Pradesh and Rajasthan, without increase in funding allocation for diagnostics in the states. This shows a direct impact for our customers (state governments) and beneficiaries (patients) sustainable over a long period of time.
Based on current timeline projection, we're targeting sales of 1 Million cartridges by end of 2024, and sales of 100 Medupi readers by end of 2024. While we continue to cultivate contacts with state health officials, finding channels to purchase and approval departments (in India and outside India) is something we can use MIT SOLVE community's help with.
For scale, there were 8.2 million microscopy based test and 2.3 million NAAT based tests done in India - This is the size of the current total addressable market which is slated to grow 5 times by the government's current estimation. We hope to start with pilots in 2 states, before expanding to other states and finally to the national TB program. The number of new patients in India was about 1.9 million in 2021. Worldwide, there were about 10 million patients.
- Government (B2G)
As explained before, the overall long strategy is to start with the Indian market, and then expand to South Africa.

We're currently bootstrapping, as planned, to finish phase I (i.e. collect field efficacy data at YRG, Chennai). Once field efficacy data is in, we'll get back to various India based grant funding partners we've been in touch with. We also plan to hire a full-time "grants-person" to help us with actively pursuing grants as we transition towards Phase II activities. Towards our bootstrapping strategy, our company has been and continues to provide consulting services to the National Institutes of Health's (NIH) Rapid Acceleration of Diagnostics (RADx) initiative.
From a product perspective, the strategy is to pursue separate approval paths for the cartridge and the whole Medupi system. The cartridge is a relatively simpler and lower cost product that we already have a lot of buy in for. It also has a lower regulatory burden, as per the Central Drugs Standard Control Organization's (India's medical devices regulatory body) guidelines and has extreme utility for the equipment used by the Indian TB program now, and for the foreseeable future. The Indian government, in 2021, released an essential equipment list enumerating equipment it seeks to procure for health centers at every level - this includes microscopy equipment for TB at various levels, indicating that apart from a strategy focused on NAAT, the government is actively procuring and putting infrastructure in place for microscopy.
Since the cartridge readily works with microscopy, and dramatically increases performance, we see it as a low barrier first product that will bring in revenue in the short term, while we work on the engineering, regulatory and production scale-up phases for the Medupi reader and approvals for the overall Medupi system.
Towards our bootstrapping strategy, our company has been and continues to provide consulting services to the NIH's RADx initiative.
The company and the project raised and continues to use grants and resources from Acumen, VentureWell, The Johns Hopkins Alliance for Healthier World, Autodesk Technology Impact program, Ballard Spahr BASE program, and the Technology Accelerator Fund at the Center for Bioengineering Innovation and Design.
Overall investment in the project exceeds $250,000 at this time.
Miss